

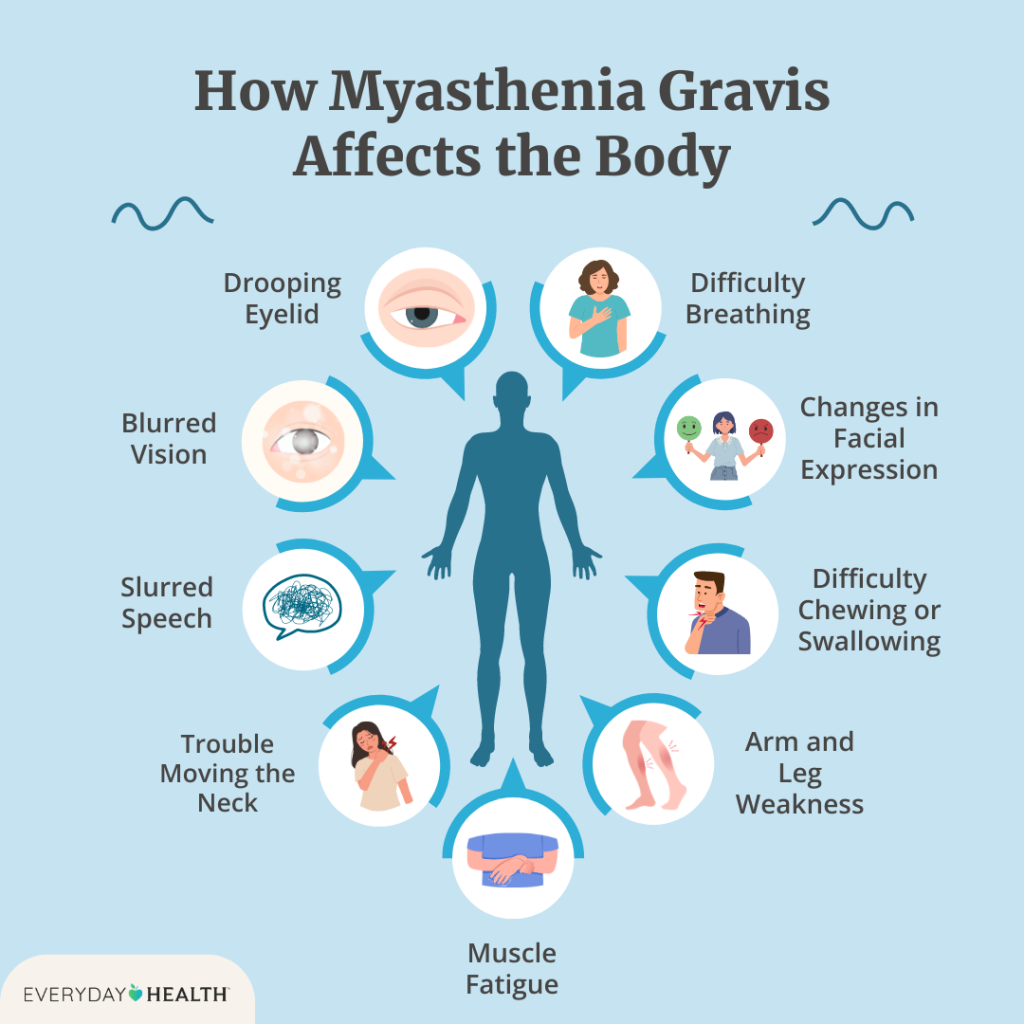
Myasthenia Gravis (MG) is a rare chronic autoimmune disorder affecting the neuromuscular junction, causing fluctuating muscle weakness and fatigue. Understanding this condition — its mechanisms, treatments, and impact on mobility — enables patients and families to optimize quality of life despite progressive symptoms.
Quick answer: Myasthenia Gravis affects 36,000–60,000 Americans (prevalence 14–20 per 100,000). It is a fatigue-based autoimmune condition where antibodies block acetylcholine receptors at the neuromuscular junction, causing muscle weakness that worsens with exertion and improves with rest. The biggest mobility lesson: energy conservation matters more than exercise. An all-terrain wheelchair isn’t “giving up” — it’s a tool that saves your energy budget for the destination instead of spending it on the walk.
1. What Causes Myasthenia Gravis?
Myasthenia Gravis is an autoimmune disorder where the body’s immune system attacks acetylcholine receptors (AChR) or related proteins at the neuromuscular junction. This prevents normal muscle contraction, resulting in weakness that worsens with activity and improves with rest.
Contributing Factors:
- Thymus Gland Abnormalities: 80% of MG patients have thymic pathology (hyperplasia or thymoma); thymus cells may drive the autoimmune response.
- Seronegative MG: Some patients lack detectable AChR antibodies but have antibodies against muscle-specific kinase (MuSK) or other proteins.
- Environmental or Infectious Triggers: Certain infections or medications may precipitate symptom onset or exacerbations.
2. How Common Is Myasthenia Gravis?
MG is rare, affecting approximately 14–20 per 100,000 people worldwide. In the United States, an estimated 36,000–60,000 individuals are living with the condition. Two age peaks are notable: women typically develop MG between ages 20–40, while men show peak onset between ages 60–80. The condition affects both sexes, though younger-onset MG is more common in women.
3. What Treatments Are Available?
While MG has no cure, multiple treatment approaches effectively manage symptoms and improve quality of life:
- Anticholinesterase Inhibitors: Pyridostigmine is first-line therapy, prolonging the availability of acetylcholine at the neuromuscular junction by inhibiting its breakdown.
- Immunosuppressive Therapy: Corticosteroids (prednisone), azathioprine, and mycophenolate mofetil reduce antibody production and immune activation.
- Plasma Exchange (Plasmapheresis): Rapidly removes pathogenic antibodies; used for crisis or pre-operatively; provides temporary relief.
- Intravenous Immunoglobulin (IVIG): Alternative or adjunctive therapy that dampens immune response; effective for acute exacerbations.
- Thymectomy: Surgical removal of the thymus gland improves symptoms in approximately 30–40% of patients, particularly those with seronegative or early-onset MG.
- Monoclonal Antibodies: Eculizumab and other newer agents target complement pathways or immune checkpoints.
4. How Does MG Affect Families?
Myasthenia Gravis creates substantial demands on family systems and support networks:
- Unpredictability: Symptoms fluctuate daily and hourly; family members must adapt to changing limitations and energy levels.
- Caregiving Load: Spouses and family members often manage medical appointments, medication schedules, and physical support.
- Financial Impact: Medication costs, therapies, specialist visits, and potential loss of income accumulate over time.
- Lifestyle Modifications: Heat, stress, and overexertion trigger flares; families must modify activities and manage environmental factors.
5. Can MG Require Assistive Mobility Devices?
Yes. In severe or generalized MG, muscle weakness can limit walking and standing endurance. Fatigue and weakness — particularly in the legs — may necessitate wheelchair use, especially for longer distances or when symptoms are poorly controlled. The variable nature of MG means mobility needs may fluctuate; some days patients walk independently, while on others they require a wheelchair or other assistive device. All-terrain wheelchairs enable safe outdoor participation without exertion.
→ The Energy-Budget Reality
Anyone who lives with MG knows it: you wake up with a fixed amount of energy, and every step uses it up. Walking a quarter-mile from the parking lot to the trailhead can cost you the rest of the afternoon. By the time you reach the view, you’re too exhausted to enjoy it.
An all-terrain wheelchair isn’t “giving up.” It’s a tool that saves your energy budget for the destination, not the walk there. The Extreme Motus is caretaker-pushed, so the rider expends near-zero energy getting to wherever the family is going. Three large balloon tires roll over sand, gravel, and trails so a partner or family member can push without the chair sticking. The result: you arrive fresh enough to actually enjoy where you went.
6. Why Is Outdoor Activity Important in MG Management?
Outdoor engagement supports comprehensive MG management:
- Mental Health: Nature reduces stress and anxiety — significant triggers for MG flares. Psychological well-being improves symptom management.
- Gentle Movement: Light outdoor activity maintains circulation and prevents deconditioning without triggering overexertion-induced weakness.
- Vitamin D Synthesis: Sunlight increases vitamin D, supporting bone health and immune regulation — particularly important for autoimmune conditions.
- Social Engagement: Community connection and shared activities reduce isolation and depression associated with chronic illness.
- Mindfulness & Stress Reduction: Nature-based mindfulness lowers stress markers that can exacerbate MG symptoms.
A note on heat & humidity
Heat is a well-documented MG trigger — even brief overheating can cause a flare. This is one reason an open-air manual chair like the Motus tends to work better than a sealed indoor power chair for MG patients who want to be outside: better airflow, no battery heat, and easy to pause in the shade. Plan outings for cooler parts of the day when possible (early morning, late afternoon, shaded trails), bring extra water, and rest before you feel exhausted, not after.
7. How All-Terrain Wheelchairs Enable Independence
For individuals with MG-related mobility limitations, all-terrain wheelchairs transform access and participation:
- Energy Conservation: Eliminates physical exertion, preserving muscle function for essential daily activities and quality time with family.
- Terrain Navigation: Handles sand, gravel, grass, trails, and uneven surfaces — removing barriers to parks, beaches, hiking trails, and nature.
- Stability & Safety: Shock-absorbing suspension and secure frame prevent jarring movements; reduces risk of falls during fatigue episodes.
- Flexibility: Accommodates the fluctuating nature of MG; users can enjoy longer outings without symptoms worsening.
- Social Inclusion: Enables participation in family outings, community events, and social gatherings — protecting psychological well-being.
- Autonomy: User-friendly design empowers independent navigation and decision-making about activities and distance.
→ See all 59 locations on our interactive map
Want to try a Motus before you commit? Several parks, zoos, and adaptive sports programs across the US, Canada, Australia, and the UK let you test-drive one on real terrain — most are free with a reservation. Find a location near you on our map →
Worried about cost? Three real funding paths.
Medical bills are already a lot for MG patients. Most families don’t pay for an all-terrain wheelchair out of pocket. Here are the funding paths customers use:
- Grants Finder — 90-second quiz that narrows 50+ adaptive-equipment grants to the ones you’re most likely to win.
- 11 Best Grants for All-Terrain Wheelchairs — full list of disability-focused grants with eligibility, deadlines, and application steps.
- Why Medicare won’t cover it (and what to do) — Medicare classifies all-terrain chairs as recreational. State Medicaid HCBS waivers and 0% interest payment plans are the workarounds.
Frequently Asked Questions About Myasthenia Gravis
Is Myasthenia Gravis hereditary?
While autoimmune susceptibility can run in families, MG is not directly inherited. Genetic predisposition may increase risk, but environmental triggers are necessary for disease onset. If a parent has MG, children have slightly elevated risk of developing MG or other autoimmune conditions, but inheritance is not guaranteed.
What is a myasthenic crisis?
A myasthenic crisis is a life-threatening emergency where muscle weakness progresses to respiratory failure, requiring mechanical ventilation. Triggers include infection, medication changes, stress, or surgery. Crisis occurs in 15–20% of MG patients. Plasma exchange and IVIG can rapidly improve crisis; recognition and immediate treatment are critical.
Is heat bad for Myasthenia Gravis?
Yes. Heat is a well-known MG trigger — overheating causes muscle weakness to worsen and can precipitate flares. This is why open-air manual all-terrain chairs (like the Extreme Motus) are often a better fit than sealed indoor power chairs for MG patients who want to be outside: better airflow, easy to rest in shade, no battery heat. Plan outings for cooler parts of the day, hydrate well, and rest preemptively.
Can I use a motorized wheelchair for MG?
Yes — and many MG patients do, particularly when in-home mobility is the primary need. Powered chairs preserve energy and Medicare often covers them with proper documentation (face-to-face evaluation, prior authorization). However, for outdoor and off-road activities, a manual all-terrain wheelchair pushed by a caregiver is often more practical: no battery to worry about in heat, no charging logistics, lighter weight, and easier transport. Many MG households use both — a powered chair for daily life, an all-terrain chair for trips and outdoor time.
Can MG be cured?
There is currently no cure for MG, but the condition is highly treatable. With modern medications and therapies, 80–90% of patients achieve good symptom control or remission. Thymectomy offers curative potential in select cases, particularly early-onset disease with thymoma.
What medications make MG worse?
Certain medications worsen MG symptoms and should be avoided: beta-blockers, fluoroquinolone antibiotics, aminoglycosides, antiarrhythmic drugs, and some anesthetics. Patients should always inform healthcare providers of their MG diagnosis before starting new medications.
How is MG diagnosed?
Diagnosis combines clinical history, physical examination (including fatigability testing), serological testing for AChR and MuSK antibodies, and electrodiagnostic studies (electromyography or repetitive nerve stimulation). MRI or CT imaging of the chest identifies thymic pathology.
How much does an all-terrain wheelchair cost for MG patients?
The Extreme Motus all-terrain wheelchair is $4,500 in 2026. Medicare won’t cover it (classified as recreational), but disability-focused grants, state Medicaid HCBS waivers, and 0% interest payment plans can bring the out-of-pocket cost down significantly. See our 2026 price guide for the full comparison vs. other manual all-terrain chairs.
Conclusion: MG doesn’t have to end your outdoor life
Myasthenia Gravis is a manageable chronic autoimmune condition. With appropriate treatment, lifestyle modifications, and the right tools, most patients maintain active, fulfilling lives. The key insight that’s often missing from medical literature: the goal isn’t pushing through the fatigue, it’s spending your energy budget on what matters.
An all-terrain wheelchair isn’t a last resort. It’s an energy-conservation tool that lets you save your strength for the view, the conversation, the family lunch at the picnic table — instead of the walk to get there.
Save your energy for the destination.
If MG is changing what your outdoor life looks like, the Motus is built for the energy budget you actually have.
Ryan Grassley · ryan@extrememotus.com


